One of the reasons, perhaps, that a lot of folks are not following the current best practices for covid risk reduction is that they have not updated their basic beliefs. A lot of things have changed. Either the earlier information turned out to be wrong, or the virus itself has changed.
So here is my list of the top ten covid myths - debunked (not in any order of importance), along with links to the past blog posts or other references.
1. I already had covid, so now I’m immune. ==> Probably wrong. “Natural immunity” doesn’t last forever. I’ve seen verified reports of as little as 23 days time until a second, separate infection. With Omicron. Or for some people, it could be as long as six months or more. I’m going to assume three months because that’s what the NFL assumed with Omicron. See Jan. 27th post.
2. I’ve been vaccinated/boosted, so now I’m immune. ==> Probably wrong. The vaccinations that we got in early 2021 are now over a year old. One can deduce that the CDC thinks there’s not much protection left from these shots, since you are eligible for a booster after five months. And another booster after only four months. See Apr. 19th post.
3. To make my event safer, I need to require all attendees to have proof of vaccination or boosting. ==> This makes no sense to me. Except for the small number of people who will have had shots within the last four or five months, it won’t appreciably reduce the risk to the group.
4. Eating inside in restaurants must be OK since they are letting us do it. ==> It’s a value judgment whether it’s OK, that is, worth the risk. It’s a fact that in a large study in 11 cities, the number of covid-19 cases was more than double in the cities allowing inside dining. See Dec. 15th post.
5. It’s got to be one or the other: masks are really good at reducing risk, and worth the bother - OR - masks aren’t much good at all and not worth the bother. ==> Both true! If you wear a tight-fitting, N95 mask, it’s going to reduce your risk a lot—I figure it as a factor of ten. If you wear a surgical mask (always gaping holes at the side) or a cloth face covering that doesn’t fit very well, it’s not going to do much good. For example, a large study of the covid-19 infections compared schools with and without mask mandates, and found that masks reduced the case rate by about 25%. See Mar. 10th post.
6. It doesn’t matter about being inside or outside—I can just stay six feet away from everyone and I’ll be OK. ==> Wrong on both counts. Being outside is the safest possible environment—there are hardly any documented cases of transmission via the outside air, and a computer simulation just made the same point (see May 20th post). And the myth about six feet was busted over a year ago, yet you still see lots of places with plexiglass barriers whenever people have to be closer together than the magical six feet. Maybe that’s fine as a feel-good measure, but it does make it hard to hear. See Nov. 24th post.
7. I feel the air blowing on me from some kind of air conditioning or fan system, so that must be doing something to make the air safe and free of viruses. ==> USUALLY WRONG! Most of the air being blown around is just recirculated air from within the room or from nearby rooms also, all mixed together. For the air conditioning units you see hanging on the walls, that’s ALL it is—no fresh outside air (virus-free) at all! This air will include all the exhaled virus from infected people currently in the room, PLUS the lingering virus from those who have been in the room recently. See Feb. 16th post.
8. There’s no way to tell in real time whether the air is full of covid-19 virus. ==> Technically true, but there is an excellent substitute, readily available. And that is to use an accurate carbon dioxide meter, from which you can determine the amount of true fresh air per person in the room. The more incoming fresh air (and corresponding exhaust air), the less virus, and vice versa. With the Safetulator™ Fresh Air Meters available on this website, you get a simple green-yellow-red assessment of the air in real time. See Apr. 29th post.
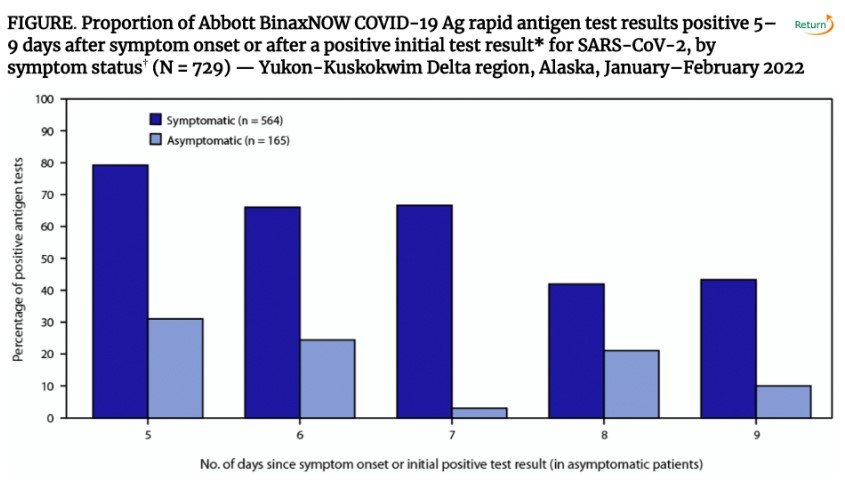
9. If I think I might have covid-19, I’ll just take a home antigen test, and if the result is negative, then I’m in the clear. ==> Wrong. Or often wrong, to be exact. With Omicron, a negative result from an antigen test is wrong about a third of the time! A positive result can be trusted, but a negative one is about like not having taken a test at all. Do you want to go out into the world with a one-third chance of spreading the virus to the people around you? But good news—you can make the test accurate by retaking it 24 hours later (and even better, a third time after another 24 hours). With multiple negative tests, it’s a good chance this is the correct result. See Feb. 2nd post.
10. It’s no big deal if I get Omicron because it has turned out to be a mild disease anyway. ==> Probably wrong. Yes, early reports speculated/hoped that this was the case. Further studies found that Omicron can be more deadly. The latest study with this conclusion was from Massachusetts, so was this a regional result, or perhaps just the first example of a more rigorous investigation? And even a mild case can lead to “long-covid” (more on this in a future blog post). NBC.com 5/20/2022